Journal of Traditional Chinese Medicine ›› 2025, Vol. 45 ›› Issue (5): 1119-1126.DOI: 10.19852/j.cnki.jtcm.2025.05.017
• Original Articles • Previous Articles Next Articles
Effectiveness of Yiqi Chupi powder (益气除疲散) for alleviating cancer-related fatigue in patients following colorectal cancer surgery: a randomized controlled trial
HAO Shulan( ), NAN Peng, LIU Likun, LI Xiaoli, ZHONG Qiming, GAO Yu, WANG Xixing(), NIE Yingfang
), NAN Peng, LIU Likun, LI Xiaoli, ZHONG Qiming, GAO Yu, WANG Xixing(), NIE Yingfang
- Shanxi Province Academy of Traditional Chinese Medicine & Shanxi Province Hospital of Traditional Chinese Medicine, Taiyuan 030012, China
-
Received:2024-09-22Accepted:2025-01-14Online:2025-10-15Published:2025-09-15 -
Contact:HAO Shulan, Shanxi Province Academy of Traditional Chinese Medicine & Shanxi Province Hospital of Traditional Chinese Medicine, Taiyuan 030012, China. dxl328321@163.com;
WANG Xixing, Shanxi Province Academy of Traditional Chinese Medicine & Shanxi Province Hospital of Traditional Chinese Medicine, Taiyuan 030012, China angxx315@163.com, Telephone: +86-13834156416
Cite this article
HAO Shulan, NAN Peng, LIU Likun, LI Xiaoli, ZHONG Qiming, GAO Yu, WANG Xixing, NIE Yingfang. Effectiveness of Yiqi Chupi powder (益气除疲散) for alleviating cancer-related fatigue in patients following colorectal cancer surgery: a randomized controlled trial[J]. Journal of Traditional Chinese Medicine, 2025, 45(5): 1119-1126.
share this article
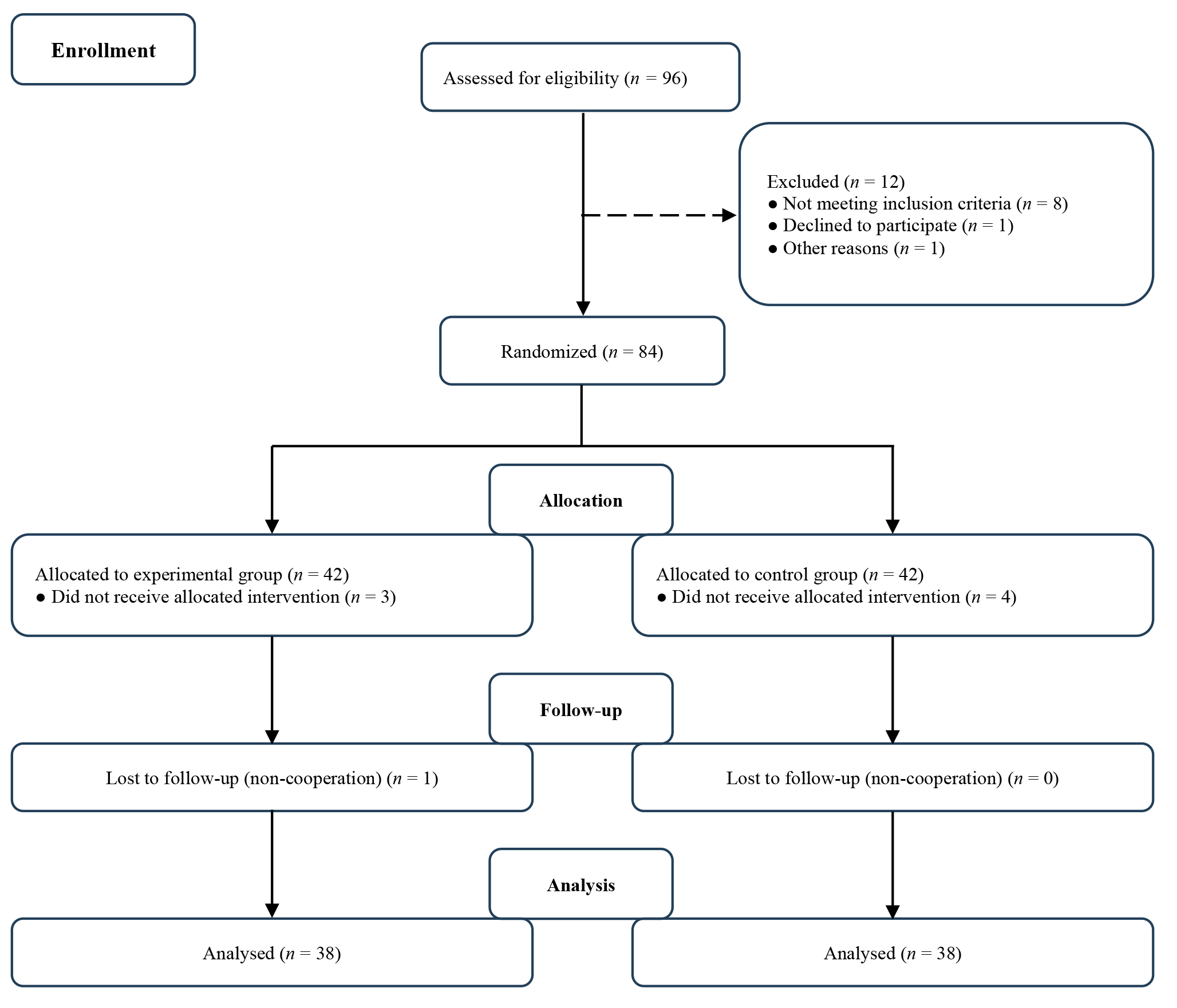
Figure 1 Study design flow diagram
Figure 1 Study design flow diagram
Table 1 Demographic and clinical characteristics
| Characteristic | Control group (n = 38) | Experimental group (n = 38) | Z/χ 2value | P value |
|---|---|---|---|---|
| Age (years) [median (Q1, Q3)] | 65 (61.75, 69) | 63 (52, 67.25) | -1.915 | 0.55 |
| Gender [n (%)] | 1.90 | 0.17 | ||
| Male | 23 (60.5) | 17 (44.7) | ||
| Female | 15 (39.5) | 21 (55.3) | ||
| Stage at cancer diagnosis [n (%)] | -1.915 | 0.55 | ||
| Lower (Ⅰ-Ⅱ) | 15 (39.5) | 9 (23.7) | ||
| Higher (Ⅲ) | 23 (60.5) | 29 (76.3) | ||
| Cancer site [n (%)] | 0.482 | 0.488 | ||
| Colon | 23 (60.5) | 20 (52.6) | ||
| Rectum | 15 (39.5) | 18 (47.4) | ||
| Differentiation (grade) [n (%)] | 0.868 | 0.868 | ||
| Low | 3 (7.9) | 4 (10.5) | ||
| Medium | 25 (65.8) | 27 (71.1) | ||
| High | 2 (5.3) | 1 (2.6) | ||
| Medium low | 5 (13.2) | 5 (13.2) | ||
| Medium high | 3 (7.9) | 1 (2.6) |
Table 1 Demographic and clinical characteristics
| Characteristic | Control group (n = 38) | Experimental group (n = 38) | Z/χ 2value | P value |
|---|---|---|---|---|
| Age (years) [median (Q1, Q3)] | 65 (61.75, 69) | 63 (52, 67.25) | -1.915 | 0.55 |
| Gender [n (%)] | 1.90 | 0.17 | ||
| Male | 23 (60.5) | 17 (44.7) | ||
| Female | 15 (39.5) | 21 (55.3) | ||
| Stage at cancer diagnosis [n (%)] | -1.915 | 0.55 | ||
| Lower (Ⅰ-Ⅱ) | 15 (39.5) | 9 (23.7) | ||
| Higher (Ⅲ) | 23 (60.5) | 29 (76.3) | ||
| Cancer site [n (%)] | 0.482 | 0.488 | ||
| Colon | 23 (60.5) | 20 (52.6) | ||
| Rectum | 15 (39.5) | 18 (47.4) | ||
| Differentiation (grade) [n (%)] | 0.868 | 0.868 | ||
| Low | 3 (7.9) | 4 (10.5) | ||
| Medium | 25 (65.8) | 27 (71.1) | ||
| High | 2 (5.3) | 1 (2.6) | ||
| Medium low | 5 (13.2) | 5 (13.2) | ||
| Medium high | 3 (7.9) | 1 (2.6) |
Table 2 Cancer-related fatigue outcomes over 12 weeks [median (Q1, Q3)]
| PFS questionnaire | Control group (n = 38) | Experimental group (n = 38) | Z value | P value |
|---|---|---|---|---|
| Behavior/daily life CRF | ||||
| Day 0 | 18.5 (13, 29) | 19 (14.75, 36) | -1.019 | 0.308 |
| Follow-up at 3 weeks | 20 (17, 32) | 19 (16, 32.25) | -0.484 | 0.628 |
| Follow-up at 6 weeks | 25 (20.75, 33) | 22 (14, 25) | -2.488 | 0.013 |
| Follow-up at 9 weeks | 27 (21, 33.25) | 22 (10.5, 25.25) | -3.702 | 0.000 |
| Follow-up at 12 weeks | 29.5 (16.75, 38) | 16 (8, 21) | -4.284 | 0.000 |
| Emotional/affective CRF | ||||
| Day 0 | 15 (11, 30.25) | 17 (12, 33.25) | -0.994 | 0.320 |
| Follow-up at 3 weeks | 18 (13, 29.25) | 16.5 (11.75, 26.75) | -1.024 | 0.306 |
| Follow-up at 6 weeks | 22 (17, 29.5) | 18 (10.75, 24.25) | -2.225 | 0.026 |
| Follow-up at 9 weeks | 24 (18, 31) | 19.5 (7.75, 23) | -3.167 | 0.002 |
| Follow-up at 12 weeks | 25 (13.75, 32.25) | 14 (5.75, 19.25) | -4.025 | 0.000 |
| Sensory/physical CRF | ||||
| Day 0 | 24.5 (16, 43) | 27.5 (17, 51) | -1.201 | 0.230 |
| Follow-up at 3 weeks | 28.5 (21.75, 45.5) | 26 (21, 42.25) | -0.738 | 0.460 |
| Follow-up at 6 weeks | 36 (27, 49.5) | 29 (15.75, 37.25) | -2.386 | 0.017 |
| Follow-up at 9 weeks | 38.5 (30, 46) | 28.5 (12.75, 36) | -3.503 | 0.000 |
| Follow-up at 12 weeks | 38.5 (22, 51.5) | 22.5 (12.25, 29.25) | -3.502 | 0.000 |
| Cognitive CRF | ||||
| Day 0 | 5 (4, 9) | 4.5 (4, 9) | -0.096 | 0.923 |
| Follow-up at 3 weeks | 6 (4, 8.25) | 4 (3, 8) | -2.039 | 0.041 |
| Follow-up at 6 weeks | 7 (4, 11) | 4 (3, 7.5) | -2.475 | 0.013 |
| Follow-up at 9 weeks | 8 (4, 11) | 4 (3, 8.25) | -2.638 | 0.008 |
| Follow-up at 12 weeks | 8 (4, 11.25) | 4 (3, 7.5) | -3.144 | 0.002 |
| Total CRF | ||||
| Day 0 | 62.5 (43.75, 109.5) | 72 (49.25, 123.5) | -1.133 | 0.257 |
| Follow-up at 3 weeks | 72 (58.75, 115) | 70.5 (53, 108) | -0.883 | 0.377 |
| Follow-up at 6 weeks | 93 (74, 114.5) | 80.5 (46.25, 94) | -2.458 | 0.014 |
| Follow-up at 9 weeks | 96.5 (80.5, 120.75) | 78.5 (33, 94.5) | -3.33 | 0.001 |
| Follow-up at 12 weeks | 106.5 (60.25, 129.75) | 62.5 (29.25, 73.5) | -3.897 | 0.000 |
Table 2 Cancer-related fatigue outcomes over 12 weeks [median (Q1, Q3)]
| PFS questionnaire | Control group (n = 38) | Experimental group (n = 38) | Z value | P value |
|---|---|---|---|---|
| Behavior/daily life CRF | ||||
| Day 0 | 18.5 (13, 29) | 19 (14.75, 36) | -1.019 | 0.308 |
| Follow-up at 3 weeks | 20 (17, 32) | 19 (16, 32.25) | -0.484 | 0.628 |
| Follow-up at 6 weeks | 25 (20.75, 33) | 22 (14, 25) | -2.488 | 0.013 |
| Follow-up at 9 weeks | 27 (21, 33.25) | 22 (10.5, 25.25) | -3.702 | 0.000 |
| Follow-up at 12 weeks | 29.5 (16.75, 38) | 16 (8, 21) | -4.284 | 0.000 |
| Emotional/affective CRF | ||||
| Day 0 | 15 (11, 30.25) | 17 (12, 33.25) | -0.994 | 0.320 |
| Follow-up at 3 weeks | 18 (13, 29.25) | 16.5 (11.75, 26.75) | -1.024 | 0.306 |
| Follow-up at 6 weeks | 22 (17, 29.5) | 18 (10.75, 24.25) | -2.225 | 0.026 |
| Follow-up at 9 weeks | 24 (18, 31) | 19.5 (7.75, 23) | -3.167 | 0.002 |
| Follow-up at 12 weeks | 25 (13.75, 32.25) | 14 (5.75, 19.25) | -4.025 | 0.000 |
| Sensory/physical CRF | ||||
| Day 0 | 24.5 (16, 43) | 27.5 (17, 51) | -1.201 | 0.230 |
| Follow-up at 3 weeks | 28.5 (21.75, 45.5) | 26 (21, 42.25) | -0.738 | 0.460 |
| Follow-up at 6 weeks | 36 (27, 49.5) | 29 (15.75, 37.25) | -2.386 | 0.017 |
| Follow-up at 9 weeks | 38.5 (30, 46) | 28.5 (12.75, 36) | -3.503 | 0.000 |
| Follow-up at 12 weeks | 38.5 (22, 51.5) | 22.5 (12.25, 29.25) | -3.502 | 0.000 |
| Cognitive CRF | ||||
| Day 0 | 5 (4, 9) | 4.5 (4, 9) | -0.096 | 0.923 |
| Follow-up at 3 weeks | 6 (4, 8.25) | 4 (3, 8) | -2.039 | 0.041 |
| Follow-up at 6 weeks | 7 (4, 11) | 4 (3, 7.5) | -2.475 | 0.013 |
| Follow-up at 9 weeks | 8 (4, 11) | 4 (3, 8.25) | -2.638 | 0.008 |
| Follow-up at 12 weeks | 8 (4, 11.25) | 4 (3, 7.5) | -3.144 | 0.002 |
| Total CRF | ||||
| Day 0 | 62.5 (43.75, 109.5) | 72 (49.25, 123.5) | -1.133 | 0.257 |
| Follow-up at 3 weeks | 72 (58.75, 115) | 70.5 (53, 108) | -0.883 | 0.377 |
| Follow-up at 6 weeks | 93 (74, 114.5) | 80.5 (46.25, 94) | -2.458 | 0.014 |
| Follow-up at 9 weeks | 96.5 (80.5, 120.75) | 78.5 (33, 94.5) | -3.33 | 0.001 |
| Follow-up at 12 weeks | 106.5 (60.25, 129.75) | 62.5 (29.25, 73.5) | -3.897 | 0.000 |
Table 3 Comparison of TCM syndrome scores and total effective rate between the two groups
| Variable | Control group (n = 38) | Experimental group (n = 38) | χ 2 value | P value |
|---|---|---|---|---|
| TCM syndrome scores [median (Q1, Q3)] | ||||
| Day 0 | 18 (16, 20.25) | 19.5 (17, 22.25) | -1.581 | 0.114 |
| Follow-up at 3 weeks | 17 (15, 20.25) | 18 (15, 20) | -0.439 | 0.661 |
| Follow-up at 6 weeks | 20 (16.75, 22) | 16 (14, 17.25) | -3.418 | 0.001 |
| Follow-up at 9 weeks | 20 (15, 23) | 14 (12.75, 16) | -4.5 | 0.001 |
| Follow-up at 12 weeks | 17 (14, 21.25) | 12 (9.75, 15) | -4.904 | 0.001 |
| TCM syndrome effective rate [n (%)] | 44.75 | < 0.01 | ||
| Healed | 0 | 3 (7.89) | ||
| Markedly effective | 0 | 3 (7.89) | ||
| Effective | 3 (7.89) | 26 (68.42) | ||
| Ineffective | 35 (92.11) | 6 (15.79) | ||
| Total effective rate | 3 (7.89) | 32 (84.21) |
Table 3 Comparison of TCM syndrome scores and total effective rate between the two groups
| Variable | Control group (n = 38) | Experimental group (n = 38) | χ 2 value | P value |
|---|---|---|---|---|
| TCM syndrome scores [median (Q1, Q3)] | ||||
| Day 0 | 18 (16, 20.25) | 19.5 (17, 22.25) | -1.581 | 0.114 |
| Follow-up at 3 weeks | 17 (15, 20.25) | 18 (15, 20) | -0.439 | 0.661 |
| Follow-up at 6 weeks | 20 (16.75, 22) | 16 (14, 17.25) | -3.418 | 0.001 |
| Follow-up at 9 weeks | 20 (15, 23) | 14 (12.75, 16) | -4.5 | 0.001 |
| Follow-up at 12 weeks | 17 (14, 21.25) | 12 (9.75, 15) | -4.904 | 0.001 |
| TCM syndrome effective rate [n (%)] | 44.75 | < 0.01 | ||
| Healed | 0 | 3 (7.89) | ||
| Markedly effective | 0 | 3 (7.89) | ||
| Effective | 3 (7.89) | 26 (68.42) | ||
| Ineffective | 35 (92.11) | 6 (15.79) | ||
| Total effective rate | 3 (7.89) | 32 (84.21) |
Table 4 Comparison of KPS score between the two groups [n (%)]
| Time point | Outcome | Control group (n = 38) | Experimental group (n = 38) | Z value | P value |
|---|---|---|---|---|---|
| Follow-up at 3 weeks | Improvement | 12 (31.6) | 13 (34.2) | 1.370 | 0.612 |
| Stable | 21 (55.3) | 23 (60.5) | |||
| Decline | 5 (13.2) | 2 (5.3) | |||
| Follow-up at 6 weeks | Improvement | 13 (34.2) | 17 (44.7) | 12.819 | 0.002 |
| Stable | 12 (31.6) | 20 (52.6) | |||
| Decline | 13 (34.2) | 1 (2.6) | |||
| Follow-up at 9 weeks | Improvement | 8 (21.1) | 21 (55.3) | 11.693 | 0.003 |
| Stable | 16 (42.1) | 13 (34.2) | |||
| Decline | 14 (36.8) | 4 (10.5) | |||
| Follow-up at 12 weeks | Improvement | 7 (18.4) | 18 (47.4) | 13.860 | 0.001 |
| Stable | 15 (39.5) | 17 (44.7) | |||
| Decline | 16 (42.1) | 3 (7.9) |
Table 4 Comparison of KPS score between the two groups [n (%)]
| Time point | Outcome | Control group (n = 38) | Experimental group (n = 38) | Z value | P value |
|---|---|---|---|---|---|
| Follow-up at 3 weeks | Improvement | 12 (31.6) | 13 (34.2) | 1.370 | 0.612 |
| Stable | 21 (55.3) | 23 (60.5) | |||
| Decline | 5 (13.2) | 2 (5.3) | |||
| Follow-up at 6 weeks | Improvement | 13 (34.2) | 17 (44.7) | 12.819 | 0.002 |
| Stable | 12 (31.6) | 20 (52.6) | |||
| Decline | 13 (34.2) | 1 (2.6) | |||
| Follow-up at 9 weeks | Improvement | 8 (21.1) | 21 (55.3) | 11.693 | 0.003 |
| Stable | 16 (42.1) | 13 (34.2) | |||
| Decline | 14 (36.8) | 4 (10.5) | |||
| Follow-up at 12 weeks | Improvement | 7 (18.4) | 18 (47.4) | 13.860 | 0.001 |
| Stable | 15 (39.5) | 17 (44.7) | |||
| Decline | 16 (42.1) | 3 (7.9) |
Table 5 Comparison of quality of Life between the two groups [median (Q1, Q3)]
| Variable | Control group (n = 38) | Experimental group (n = 38) | Z value | P value |
|---|---|---|---|---|
| Day 0 | 43.5 (38.75, 50) | 41 (39, 47) | -1.036 | 0.3 |
| Follow-up at 3 weeks | 44 (39.5, 51) | 46 (43, 49) | -0.947 | 0.343 |
| Follow-up at 6 weeks | 45 (39, 49) | 46.5 (43.75, 49) | -1.907 | 0.057 |
| Follow-up at 9 weeks | 45 (39.75, 48) | 48 (46, 51) | -3.531 | 0.01 |
| Follow-up at 12 weeks | 46 (39.75, 49.25) | 51 (48, 54.25) | -4.49 | 0.01 |
Table 5 Comparison of quality of Life between the two groups [median (Q1, Q3)]
| Variable | Control group (n = 38) | Experimental group (n = 38) | Z value | P value |
|---|---|---|---|---|
| Day 0 | 43.5 (38.75, 50) | 41 (39, 47) | -1.036 | 0.3 |
| Follow-up at 3 weeks | 44 (39.5, 51) | 46 (43, 49) | -0.947 | 0.343 |
| Follow-up at 6 weeks | 45 (39, 49) | 46.5 (43.75, 49) | -1.907 | 0.057 |
| Follow-up at 9 weeks | 45 (39.75, 48) | 48 (46, 51) | -3.531 | 0.01 |
| Follow-up at 12 weeks | 46 (39.75, 49.25) | 51 (48, 54.25) | -4.49 | 0.01 |
| 1. | Davidson KW, Barry MJ, Mangione CM, et al. Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA 2021; 325: 1965-77. |
| 2. | Qian JN, Xu Yan, Hu HY, Zhao AG. Clinical efficacy and safety evaluation of Buzhongyiqi pills on appetite improvement in patients with colorectal cancer receiving chemotherapy: a pilot randomized cross-over clinical trial. J Tradit Chin Med 2024; 44: 1254-67. |
| 3. | Zhang ZJ, Zhang M, Wu XT, Cui Q, Guo YJ. Zhengyuan capsule for the treatment of cancer-related fatigue in lung cancer patients undergoing operation: a study protocol for a randomized controlled trial. J Tradit Chin Med 2021; 41: 486-91. |
| 4. | Husebø AML, Dalen I, Søreide JA, Bru E, Richardson A. Cancer-related fatigue and treatment burden in surgically treated colorectal cancer patients-a cross-sectional study. J Clin Nurs 2022; 31: 3089-101. |
| 5. | Huang ST, Ke X, Yu XY, Wu YX, Huang YX, Liu D. Risk factors for cancer-related fatigue in patients with colorectal cancer: a systematic review and Meta-analysis. Support Care Cancer 2022; 30: 10311-22. |
| 6. |
Wang S, Jiang N, Song Y, et al. Correlates of cancer-related fatigue among colorectal cancer patients undergoing postoperative adjuvant therapy based on the theory of unpleasant symptoms. Curr Oncol 2022; 29: 9199-214.
DOI PMID |
| 7. | Geng L, Li X, Guo L, Zhang R, Yue S. The content and effectiveness of physical activity for cancer-related fatigue among colorectal cancer survivors: systematic review and Meta-analysis. Nurs Open 2023; 10: 4274-85. |
| 8. | Dun L, Wu XY, Huang ST. Effects of cognitive training and social support on cancer-related fatigue and quality of life in colorectal cancer survivors: a systematic review and Meta-analysis. Integr Cancer Ther 2022; 21: 15347354221081271. |
| 9. | Yang J, Li Y, Chau CI, et al. Efficacy and safety of Traditional Chinese Medicine for cancer-related fatigue: a systematic literature review of randomized controlled trials. Chin Med 2023; 18: 142. |
| 10. | Deng SM, Chiu AF, Wu SC, et al. Association between cancer-related fatigue and Traditional Chinese Medicine body constitution in female patients with breast cancer. J Tradit Complement Med 2021; 11: 62-7. |
| 11. |
Li R, Zhang T, Yan SH, et al. Chinese medicine combined with adjuvant chemotherapy for improving myelosuppression in colorectal cancer patients: a systematic review and network Meta-analysis. Chin J Integr Med 2024; 30: 643-52.
DOI PMID |
| 12. |
Yang WS, Ma YN, Smith-Warner S, et al. Calcium intake and survival after colorectal cancer diagnosis. Clin Cancer Res 2019; 25: 1980-8.
DOI PMID |
| 13. |
Fleshman J, Branda ME, Sargent DJ, et al. Disease-free survival and local recurrence for laparoscopic resection compared with open resection of stage Ⅱ to Ⅲ rectal cancer: follow-up results of the ACOSOG Z6051 randomized controlled trial. Ann Surg 2019; 269: 589-95.
DOI PMID |
| 14. |
Li Y, Gu J, Zhou H, et al. Traditional Chinese Medicine symptom patterns in patients with colorectal carcinoma. J Tradit Chin Med 2018; 38: 299-308.
PMID |
| 15. | Yoshino T, Yamanaka T, Oki E, et al. Efficacy and long-term peripheral sensory neuropathy of 3 vs 6 months of oxaliplatin-based adjuvant chemotherapy for colon cancer: the ACHIEVE phase 3 randomized clinical trial. JAMA Oncol 2019; 5: 1574-81. |
| 16. | Berardi A, Graziosi G, Ferrazzano G, et al. Evaluation of the psychometric properties of the revised piper fatigue scale in patients with multiple sclerosis. Healthcare (Basel) 2022; 10: 985. |
| 17. |
Wang Q, Jiao L, Wang S, et al. Maintenance chemotherapy with Chinese herb medicine formulas vs with placebo in patients with advanced non-small cell lung cancer after first-line chemotherapy: a multicenter, randomized, double-blind trial. Front Pharmacol 2018; 9: 1233.
DOI PMID |
| 18. |
Li Y, Sui X, Su Z, et al. Meta-analysis of paclitaxel-based chemotherapy combined with Traditional Chinese Medicines for gastric cancer treatment. Front Pharmacol 2020; 11: 132.
DOI PMID |
| 19. |
Wang H, Zhao T, Lyu C, Zhang Z, Fang F, Li B. Serum metabonomics as a diagnostic approach for cancer-related fatigue. Exp Ther Med 2022; 23: 256.
DOI PMID |
| 20. | Chi WC, Jiang QH, Jiang JK, Ma BZ. Progress in Traditional Chinese Medicine treatment of cancer-related fatigue in gastric cancer. Minerva Surg 2024; 79: 129-31. |
| 21. | Ye X, Zhang H, Li Q, Ren H, Xu X, Li X. Structural-activity relationship of rare ginsenosides from red ginseng in the treatment of Alzheimer's disease. Int J Mol Sci 2023; 24: 8625. |
| 22. | Im DS. Pro-resolving effect of ginsenosides as an anti-inflammatory mechanism of Panax Ginseng. Biomolecules 2020; 10: 444. |
| 23. |
Fan W, Huang Y, Zheng H, et al. Ginsenosides for the treatment of Metabolic syndrome and cardiovascular diseases: pharmacology and mechanisms. Biomed Pharmacother 2020; 132: 110915.
DOI PMID |
| 24. | Zhou J, Zheng F, Chen J, et al. Effect of acupoint conditioning nursing technology based on holistic view of Traditional Chinese Medicine on cancer-related fatigue of patients with lung cancer after chemotherapy. Minerva Surg 2024: 1. |
| 25. | Zhang C, Guo W, Yao X, et al. Database mining and animal experiment-based validation of the efficacy and mechanism of Radix Astragali (Huangqi) and Rhizoma Atractylodis Macrocephalae (Baizhu) as core drugs of Traditional Chinese Medicine in cancer-related fatigue. J Ethnopharmacol 2022; 285: 114892. |
| 26. | Meng M, Li X, Peng K, et al. Cultural adaptation of the pan-canadian oncology symptom triage and remote support practice guide for cancer-related fatigue in China: integration of Traditional Chinese Medicine nursing evidence. Asia Pac J Oncol Nurs 2023; 10: 100252. |
| 27. |
Ming W, Yun Z. Clinical value of modified Shenling Baizhu powder in treating targeted therapy-induced diarrhea in non-small cell lung cancer. J Tradit Chin Med 2024; 44: 1000-5.
DOI |
| 28. | Frappaz D, Bonneville-Levard A, Ricard D, et al. Assessment of Karnofsky (KPS) and WHO (WHO-PS) performance scores in brain tumour patients: the role of clinician bias. Support Care Cancer 2021; 29: 1883-91. |
| 29. | Li H, Ji Y, Zhang S, et al. Kangai injection combined with platinum-based chemotherapy for the treatment of stage Ⅲ/Ⅳ non-small cell lung cancer: a Meta-analysis and systematic review of 35 randomized controlled trials. J Cancer 2019; 10: 5283-98. |
| 30. | Huang S, Peng W, Mao D, et al. Kangai injection, a Traditional Chinese Medicine, improves efficacy and reduces toxicity of chemotherapy in advanced colorectal cancer patients: a systematic review and Meta-analysis. Evid Based Complement Alternat Med 2019; 2019: 8423037. |
| 31. |
Qi F, Zhao L, Zhou A, et al. The advantages of using Traditional Chinese Medicine as an adjunctive therapy in the whole course of cancer treatment instead of only terminal stage of cancer. Biosci Trends 2015; 9: 16-34.
DOI PMID |
| 32. |
Wang S, Sun Y, Zhang J, et al. Astragalus polysaccharides/chitosan microspheres for nasal delivery: preparation, optimization, characterization, and pharmacodynamics. Front Pharmacol 2020; 11: 230.
DOI PMID |
| 33. | Zhang X, Liang T, Yang W, et al. Astragalus membranaceus injection suppresses production of interleukin-6 by activating autophagy through the AMPK-mTOR pathway in lipopolysaccharide-stimulated macrophages. Oxid Med Cell Longev 2020; 2020: 1364147. |
| 34. |
Yang L, Li TT, Chu YT, et al. Traditional Chinese medical comprehensive therapy for cancer-related fatigue. Chin J Integr Med 2016; 22: 67-72.
DOI PMID |
| 35. |
Zhao YY, Wang SM, Li JH, Zhou YS, Wu WY, Swei Sunny H. Effectiveness and safety of traditional Chinese medical therapy for cancer-related fatigue: a systematic review and Meta-analysis of randomized controlled trials. J Tradit Chin Med 2020; 40: 738-48.
DOI |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||