Journal of Traditional Chinese Medicine ›› 2022, Vol. 42 ›› Issue (1): 140-147.DOI: 10.19852/j.cnki.jtcm.2022.01.009
• Guideline • Previous Articles Next Articles
Acupuncture for low back pain: a clinical practice guideline from the Hong Kong taskforce of standardized acupuncture practice
Haiyong CHEN1, Wing-Fai YEUNG2( ), Mingxiao YANG3, Jinglan MU4, Tat-Chi ZIEA5, Bacon Fung-Leung NG5, Lixing LAO6()
), Mingxiao YANG3, Jinglan MU4, Tat-Chi ZIEA5, Bacon Fung-Leung NG5, Lixing LAO6()
- 1 School of Chinese Medicine, University of Hong Kong, Hong Kong SAR, China
2 School of Nursing, Hong Kong Polytechnic University, Hong Kong SAR, China
3 Bendheim Integrative Medicine Center, Memorial Sloan Kettering Cancer Center, 1429 First Avenue, New York 10021, USA
4 Department of Anesthesiology, Nanjing Drum Tower Hospital, Nanjing University Medical School, Nanjing, 210008, China
5 Chinese Medicine Department, Hong Kong Hospital Authority, Hong Kong SAR, China
6 Virginia University of Integrative Medicine, Fairfax, VA 22031, USA
-
Received:2020-09-21Accepted:2020-12-08Online:2022-02-15Published:2021-01-19 -
Contact:Wing-Fai YEUNG,Lixing LAO -
About author:Dr. YEUNG Wingfai, School of Nursing, Hong Kong Polytechnic University, Hong Kong SAR, China. jerry-wf.yeung@polyu.edu.hk
Prof. LAO Lixing, Virginia University of Integrative Medicine, 9401 Mathy Drive, Fairfax, VA 22031, USA. llao@vuim.edu;
-
Supported by:Hong Kong Hospital Authority-funded Project: Development of Chinese Medicine Acupuncture Clinical Practice Guideline (CPG) in Low Back Pain(HA105/48 PT 19 (2013/14));National Center for Complementary and Integrative Health, National Institutes of Health (NIH NCCIH)-funded Project: “Cochrane Complementary Medicine Field: Resource for Research(R24 AT001293-02)
Cite this article
Haiyong CHEN, Wing-Fai YEUNG, Mingxiao YANG, Jinglan MU, Tat-Chi ZIEA, Bacon Fung-Leung NG, Lixing LAO. Acupuncture for low back pain: a clinical practice guideline from the Hong Kong taskforce of standardized acupuncture practice[J]. Journal of Traditional Chinese Medicine, 2022, 42(1): 140-147.
share this article
Table 1 Level of Evidence and Strength of Recommendations for TCM CPGs
| Level of evidence | Description |
|---|---|
| Ia | Evidence from at least two types of research as follows: randomized controlled trial, cohort study, case-control study, and case report, with the consistent effect size and direction; |
| Ⅰb | Evidence from a single randomized controlled trial with sufficient power; |
| Ⅱa | Evidence from controlled studies without randomization or cohort studies; |
| Ⅱb | Evidence from case-control studies (non-experimental descriptive study); |
| Ⅲa | Evidence from historical controlled studies (non-experimental descriptive study); |
| Ⅲb | Evidence from before-after case-control studies (non-experimental descriptive study); |
| Ⅳ | Evidence from well-known reported cases or classical traditional Chinese textbooks; |
| Ⅴ | Evidence from expert committee reports or opinions or clinical experience of respected authorities, or case report not applied widely, and therapy recorded in classical traditional Chinese textbooks but not applied in practice; |
Table 1 Level of Evidence and Strength of Recommendations for TCM CPGs
| Level of evidence | Description |
|---|---|
| Ia | Evidence from at least two types of research as follows: randomized controlled trial, cohort study, case-control study, and case report, with the consistent effect size and direction; |
| Ⅰb | Evidence from a single randomized controlled trial with sufficient power; |
| Ⅱa | Evidence from controlled studies without randomization or cohort studies; |
| Ⅱb | Evidence from case-control studies (non-experimental descriptive study); |
| Ⅲa | Evidence from historical controlled studies (non-experimental descriptive study); |
| Ⅲb | Evidence from before-after case-control studies (non-experimental descriptive study); |
| Ⅳ | Evidence from well-known reported cases or classical traditional Chinese textbooks; |
| Ⅴ | Evidence from expert committee reports or opinions or clinical experience of respected authorities, or case report not applied widely, and therapy recorded in classical traditional Chinese textbooks but not applied in practice; |
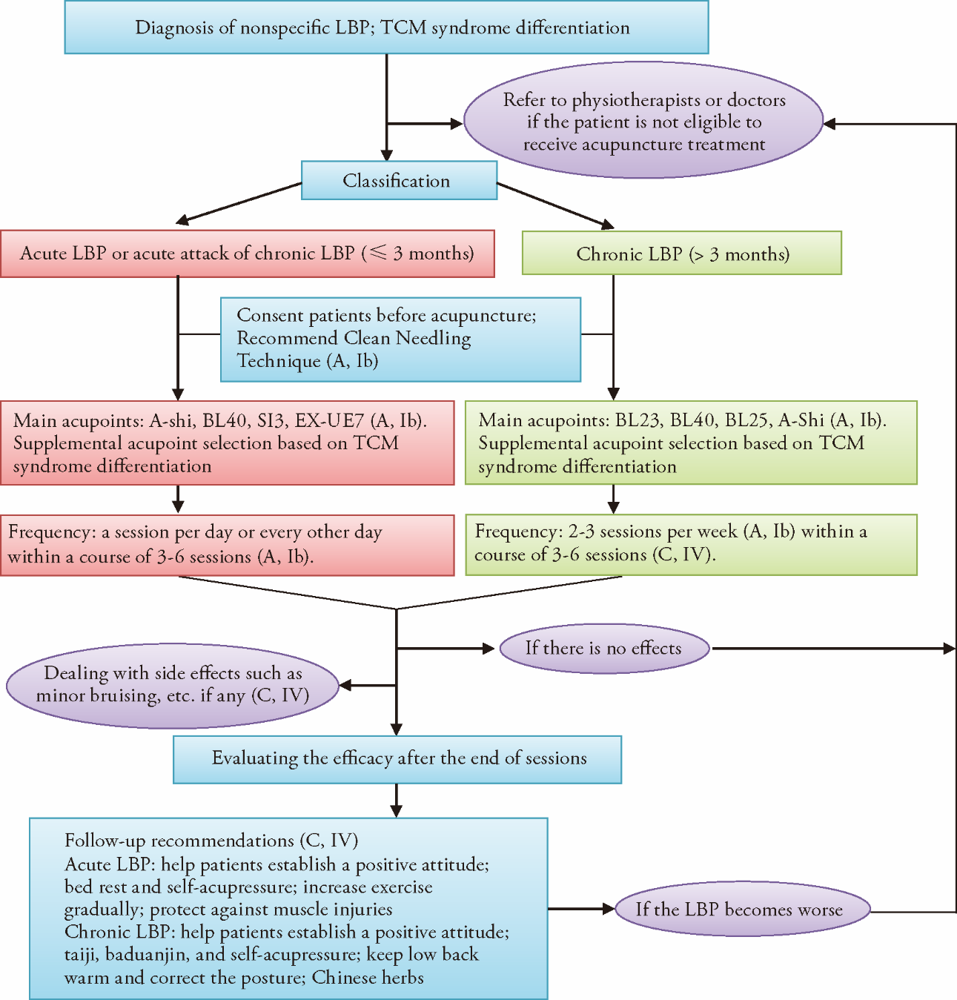
Figure 1. Recommendations on Diagnosis and Acupuncture Treatment Procedure for Low Back Pain. The recommended clinical flow and procedures on using traditional Chinese MedicineTraditional Chinese Medicine diagnosis and acupuncture to management low back pain (LBP). Grades of Recommendations: A, directly based on Level I evidence (Ia & and Ib); B, directly based on Level Ⅱ & and Ⅲ evidence; C, directly based on Level IV & and V evidence.
Figure 1. Recommendations on Diagnosis and Acupuncture Treatment Procedure for Low Back Pain. The recommended clinical flow and procedures on using traditional Chinese MedicineTraditional Chinese Medicine diagnosis and acupuncture to management low back pain (LBP). Grades of Recommendations: A, directly based on Level I evidence (Ia & and Ib); B, directly based on Level Ⅱ & and Ⅲ evidence; C, directly based on Level IV & and V evidence.
Table 2 Roadmap of recommended practice of acupuncture treatment for low back pain (LBP)
| Item | Acute LBP and acute attack of chronic LBP | Chronic LBP |
|---|---|---|
| Treatment principle | Promote Qi flow to relieve pain, relax sinews, and activate blood (C, IV). | Relax sinews and activate collaterals; unblock meridians to relieve pain; tonify kidney and spleen (C, IV). |
| Acupoints selection based on syndrome differentiation | Main acupoints: A-shi point, Weizhong (BL40), Houxi (SI3) Syndrome-based supplementary acupoints: Governor Vessel Syndrome: Shuigou (GV26) Foot Taiyang Bladder Meridian Syndrome: Kunlun (BL60) Additional acupoint: Shenmai (BL62), Yanglao (SI6), Zanzhu (BL2), Waiguan (TE5), Zulinqi (GB41), Yanglingquan (GB34) | Main acupoints: Shenshu (BL23), Weizhong (BL40), Dachangshu (BL25), A-shi point Syndrome-based supplementary acupoints: Governor Vessel Syndrome: Mingmen (GV4), Houxi (SI3), Huatuojiaji (EX-B2) Foot taiyang Bladder Meridian Syndrome: Kunlun (BL60) Cold-dampness: Yaoyangguan (GV3) (C, IV). Qi stagnation and blood stasis: Geshu (BL17) (C, IV). Kidney deficiency: Zhishi (BL52), Taixi (KI3) (C, IV). Lumbosacral pain: Ciliao (BL32), Yaochu (GV2) (C, IV). |
| Position | Usually patients are in prone position, but older patients could lie on either side. Sitting position can be used if the needle retention time is short (C, IV). | Usually patients are in prone position, but older patients could lie on either side. Sitting position can be used if the needle retention time is short (C, IV). |
| Acupuncture technique | Filiform needles [ø 0.25 mm 18(A, Ib), 1-1.5 cun (C, IV)] are recommended. First, insert needles at EX-UE7, SI3 when patient is in standing and convey strong stimulation by twirling/lifting and thrusting for 1-3 min (C, IV). Then ask patient to turn the waist slowly and remove needles after pain has been reduced. Second, if the acute pain is eased after initial treatment and local muscle in the low back area is not too stiff/tight, let patient lie prone on bed and stimulate A-shi point and Weizhong (BL40) using the bloodletting method (C, IV). | According to the excess or deficiency nature of syndromes, use the bloodletting method or reinforcing method in combination with moxibustion. Needles of 0.3 mm in diameter and 40 mm in length are recommended (C, IV). The depth of needle insertion varies depending on the location of the acupoints and the muscle thickness of patients, usually ranging from 10 to 30 mm. After insertion of needles, use a suitable technique to stimulate the acupoints to obtain the “De Qi” sensation (C, IV). |
| Duration | The needles should be retained in situ for 20-30 min at each session (C, IV). | The needles should be retained in situ for 20-30 min at each session (C, IV). |
| Treatment frequency and course | In the beginning, acupuncture treatment can be offered once a day or every other day | At the beginning, offer acupuncture two to three times a week |
Table 2 Roadmap of recommended practice of acupuncture treatment for low back pain (LBP)
| Item | Acute LBP and acute attack of chronic LBP | Chronic LBP |
|---|---|---|
| Treatment principle | Promote Qi flow to relieve pain, relax sinews, and activate blood (C, IV). | Relax sinews and activate collaterals; unblock meridians to relieve pain; tonify kidney and spleen (C, IV). |
| Acupoints selection based on syndrome differentiation | Main acupoints: A-shi point, Weizhong (BL40), Houxi (SI3) Syndrome-based supplementary acupoints: Governor Vessel Syndrome: Shuigou (GV26) Foot Taiyang Bladder Meridian Syndrome: Kunlun (BL60) Additional acupoint: Shenmai (BL62), Yanglao (SI6), Zanzhu (BL2), Waiguan (TE5), Zulinqi (GB41), Yanglingquan (GB34) | Main acupoints: Shenshu (BL23), Weizhong (BL40), Dachangshu (BL25), A-shi point Syndrome-based supplementary acupoints: Governor Vessel Syndrome: Mingmen (GV4), Houxi (SI3), Huatuojiaji (EX-B2) Foot taiyang Bladder Meridian Syndrome: Kunlun (BL60) Cold-dampness: Yaoyangguan (GV3) (C, IV). Qi stagnation and blood stasis: Geshu (BL17) (C, IV). Kidney deficiency: Zhishi (BL52), Taixi (KI3) (C, IV). Lumbosacral pain: Ciliao (BL32), Yaochu (GV2) (C, IV). |
| Position | Usually patients are in prone position, but older patients could lie on either side. Sitting position can be used if the needle retention time is short (C, IV). | Usually patients are in prone position, but older patients could lie on either side. Sitting position can be used if the needle retention time is short (C, IV). |
| Acupuncture technique | Filiform needles [ø 0.25 mm 18(A, Ib), 1-1.5 cun (C, IV)] are recommended. First, insert needles at EX-UE7, SI3 when patient is in standing and convey strong stimulation by twirling/lifting and thrusting for 1-3 min (C, IV). Then ask patient to turn the waist slowly and remove needles after pain has been reduced. Second, if the acute pain is eased after initial treatment and local muscle in the low back area is not too stiff/tight, let patient lie prone on bed and stimulate A-shi point and Weizhong (BL40) using the bloodletting method (C, IV). | According to the excess or deficiency nature of syndromes, use the bloodletting method or reinforcing method in combination with moxibustion. Needles of 0.3 mm in diameter and 40 mm in length are recommended (C, IV). The depth of needle insertion varies depending on the location of the acupoints and the muscle thickness of patients, usually ranging from 10 to 30 mm. After insertion of needles, use a suitable technique to stimulate the acupoints to obtain the “De Qi” sensation (C, IV). |
| Duration | The needles should be retained in situ for 20-30 min at each session (C, IV). | The needles should be retained in situ for 20-30 min at each session (C, IV). |
| Treatment frequency and course | In the beginning, acupuncture treatment can be offered once a day or every other day | At the beginning, offer acupuncture two to three times a week |
| [1] | Cheng L, Lau KK, Lam W, et al. Evidence-based guideline on prevention and management of low back pain in working population in primary care. Hong Kong Pract 2012;34:106-15. |
| [2] | Freburger JK, Holmes GM, Agans RP, et al. The rising prevalence of chronic low back pain. Arch Intern Med 2009;169:251-8. |
| [3] | Stanton TR, Henschke N, Maher CG, et al. After an episode of acute low back pain, recurrence is unpredictable and not as common as previously thought. Spine 2008;33:2923-8. |
| [4] | Patrick N, Emanski E, Knaub MA. Acute and chronic low back pain. Med Clin North Am 2014;98:777-89. |
| [5] | Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet 2017;389:736-47. |
| [6] | Haake M, Müller H-H, Schade-Brittinger C, et al. German Acupuncture Trials (GERAC) for chronic low back pain: randomized, multicenter, blinded, parallel-group trial with 3 groups. Arch Intern Med 2007;167:1892-8. |
| [7] | Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture for chronic pain: individual patient data Meta-analysis. Arch Intern Med 2012;172:1444-53. |
| [8] | Fan AY, Miller DW, Bolash B, et al. Acupuncture’s role in solving the opioid epidemic: evidence, cost-effectiveness, and care availability for acupuncture as a primary, non-pharmacologic method for pain relief and management-white paper 2017. J Integr Med 2017;15:411-25. |
| [9] | Liu J-P. The composition of evidence body of traditional medicine and recommendations for its evidence grading. Zhong Guo Zhong Xi Yi Jie He Za Zhi 2007;27:1061-5. |
| [10] | 20. Zhong LL, Shi N, Dai L, et al. Evidence-based Chinese medicine clinical practice guideline for stomach pain in Hong Kong. Chin J Integr Med 2017;23:793-800. |
| [11] | Shi N, Zhong LL, Han X, et al. Enhanced evidence-based Chinese medicine clinical practice guidelines in Hong Kong: a study protocol for three common diseases. Evid Based Complement Alternat Med 2015;2015:482706. |
| [12] | Scottish Intercollegiate Guidelines Network (SIGN). A guideline developer’s handbook. Edinburgh: SIGN; 2019. (SIGN publication No. 50). 2019-11, cited 2021-12-02; 67 screens. Available from URL: https://www.sign.ac.uk/media/1050/sign50_2019.pdf. |
| [13] | Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet 2012;379:482-91. |
| [14] | Xu S, Wang L, Cooper E, et al. Adverse events of acupuncture: a systematic review of case reports. Evid Based Complement Alternat Med 2013;2013:581203. |
| [15] | Council of Colleges of Acupuncture and Oriental Medicine (CCAOM). Clean Needle Technique Manual (7th Edition). 2017-05, cited 2021-12-02; 4 screens. Available from URL: https://www.ccaom.org/images/ccaom/Documents/7th_Edition_Manual_English_June_2017.pdf. |
| [16] | Shin JS, Ha IH, Lee J, et al. Effects of motion style acupuncture treatment in acute low back pain patients with severe disability: a multicenter, randomized, controlled, comparative effectiveness trial. Pain 2013;154:1030-7. |
| [17] | Lee JH, Choi TY, Lee MS, et al. Acupuncture for acute low back pain: a systematic review. Clin J Pain 2013;29:172-85. |
| [18] | Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci 2003;26:17-22. |
| [19] | Vincent C. The safety of acupuncture: acupuncture is safe in the hands of competent practitioners. BMJ 2001;323:467-8. |
| [20] | Furlan AD, Van Tulder MW, Cherkin D, et al. Acupuncture and dry-needling for low back pain. Cochrane Database Syst Rev 2005; (1): CD001351. |
| [21] | Liu Z, Liu L. Essentials of Chinese Medicine. Springer Science & Business Media, 2011. |
| [22] | Yun M, Shao Y, Zhang Y, et al. Hegu acupuncture for chronic low-back pain: a randomized controlled trial. J Altern Complement Med 2012;18:130-6. |
| [23] | Yun M, Xiong N, Guo M, et al. Acupuncture at the back-pain-acupoints for chronic low back pain of peacekeepers in Lebanon: a randomized controlled trial. J Musculoskelet Pain 2012;20:107-15. |
| [24] | Jiang GM, Lin MD, Wang LY. Comparative study on effect of acupuncture and lidocaine block for lumbar myofascial pain syndrome. Zhongguo Zhen Jiu 2013;33:223-6. |
| [25] | Brinkhaus B, Witt CM, Jena S, et al. Acupuncture in patients with chronic low back pain: a randomized controlled trial. Arch Intern Med 2006;166:450-7. |
| [26] | Kerr DP, Walsh DM, Baxter D. Acupuncture in the management of chronic low back pain: a blinded randomized controlled trial. Clin J Pain 2003;19:364-70. |
| [27] | Cherkin DC, Sherman KJ, Avins AL, et al. A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. Arch Intern Med 2009;169:858-66. |
| [28] | Witt CM, Jena S, Selim D, et al. Pragmatic randomized trial evaluating the clinical and economic effectiveness of acupuncture for chronic low back pain. Am J Epidemiol 2006;164:487-96. |
| [29] | Yu W, Xu J, Shi N, et al. Assessing the quality of the first batch of evidence-based clinical practice guidelines in Traditional Chinese Medicine. J Tradit Chin Med 2011;31:376-81. |
| [30] | Fan AY, Ouyang H, Qian X, et al. Discussions on real-world acupuncture treatments for chronic low-back pain in older adults. J Integr Med 2019;17:71-6. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||